Be prepared.
The lung cancer in most patients on whom we thoracic surgeons operate is situated entirely within a lobe of the lung and a lobectomy is a sufficient operation. Occasionally, as previously discussed, it is too large or is positioned such that an entire lung must be removed; a pneumonectomy. There are two atypical locations that necessitate additional surgical attention.
One is when the cancer invades a large airway such as the trachea (the “main” airway from the throat) or one of the bronchi (the airways from the trachea to each of the two lungs). In this instance the surgeon must be prepared to perform a lobectomy or pneumonectomy and at the same time cut out the portion of the tubular airway to which the cancer is attached. Upon completion of the cancer procedure the two open ends of the airway “tube” must be sewn back together.
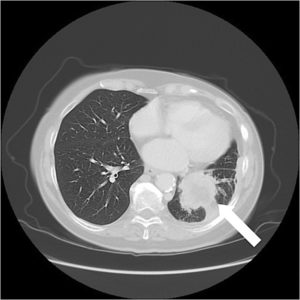
The other atypical location is when the cancer has spread through the lining of the lung (the pleura) and has invaded -grown into – the chest wall, specifically the rib cage. This situation requires that the surgeon excise enough of the rib cage to be sure all the cancer is encompassed. This usually means three or more ribs along with and still attached to the removed lobe or lung.
A thoracic surgeon is prepared for these situations, which are usually identified by preoperative tests, and can perform the necessary operations without a significant increase in morbidity or decrease in cure likelihood.



